
The healthcare worker shortage is dire, but it’s treatable
Hospitals and other providers are having to find creative ways to attract, develop, and retain people in the most critical positions. Lives depend on it.
Rob Preston | April 12, 2023

Catherine “CJ” Robison remembers the precise moment she decided to give up her career as a nurse.
It was 2018, and Robison and the understaffed team she was managing were working late nights at a 250-bed hospital, caring for patients who were sometimes packed into conference rooms during peak times. One evening at home after a long shift, having headed to bed for a few hours of sleep before planning to return to the hospital, she heard her three-month-old crying, needing to be fed. “And that was when I thought, ‘I’m done.’” says Robison, who now works in healthcare technology. “Three months later, I quit.”
“The work is harder, the patients are sicker, and it's emotionally, physically taxing on the nurses and other personnel.”
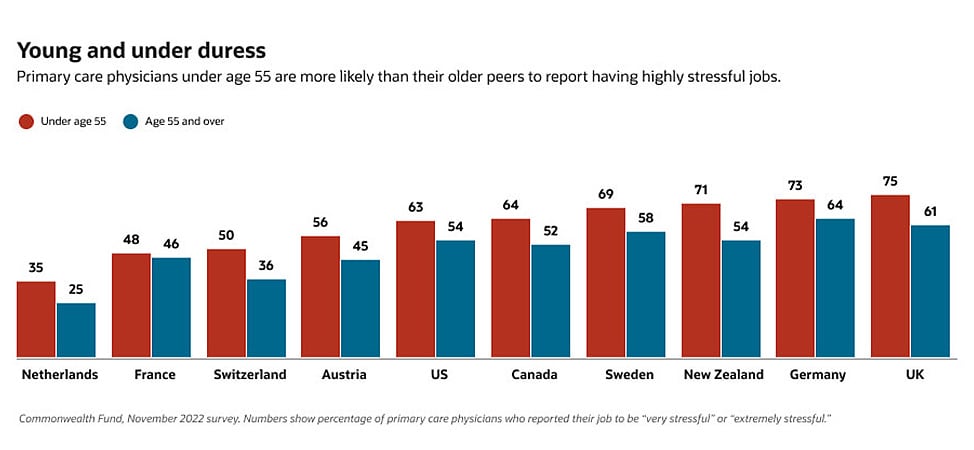
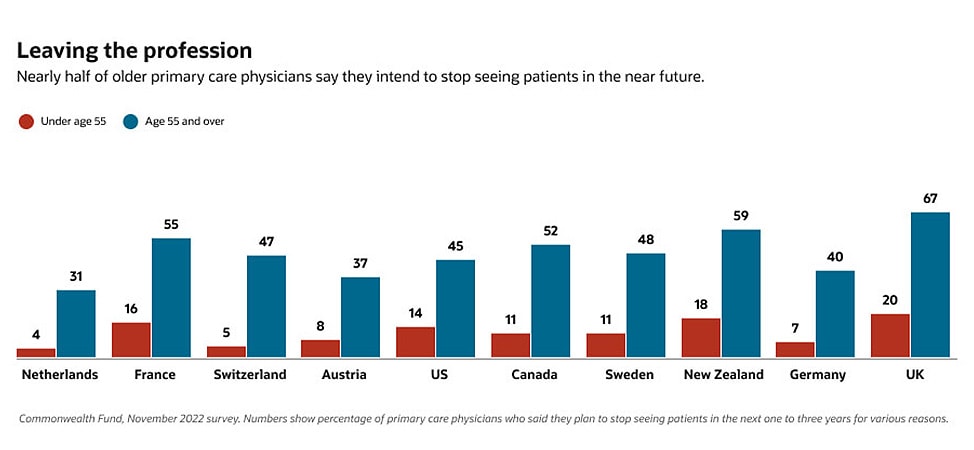
Burnout of the kind Robison experienced, only made worse by the COVID-19 pandemic, is just one of many reasons for the healthcare industry’s dire worker shortage. Other reasons include an aging workforce, with clinicians retiring faster than they can be replaced; an aging population that includes more people with chronic conditions to treat; changing disease patterns that require treatment from different kinds of scarce specialists; and insufficient numbers of graduates coming out of medical and nursing schools. Even before the pandemic stretched the global healthcare system to its breaking point, the World Health Organization was projecting a worldwide shortage of 18 million doctors, nurses, and other frontline health professionals by 2030.
The shortage of qualified personnel is now the United States healthcare industry’s number one challenge for the first time in 17 years, according to the latest annual survey by the American College of Healthcare Executives, ranking ahead of financial pressures, patient safety, behavioral health/addiction, and several other pressing issues. Some hospital systems—especially in remote areas, which have the hardest time attracting doctors, nurses, and other professionals—have had to close entire departments, including emergency care, infection control, maternity, and cardiology. A shortage of clinicians and other healthcare workers in Syracuse, New York, recently forced local hospitals to turn away thousands of patients.
In a March 2022 letter to the House Energy and Commerce Committee, the American Hospital Association (AHA) called the situation a “national emergency,” reporting that 23% of US hospitals were experiencing “severe” staffing shortages. The AHA estimates that US providers will face a shortfall of up to 124,000 physicians by 2033 and will need to hire at least 200,000 nurses every year to meet rising demands and replace those who retire or leave the profession. Compare that number to the annual number of RN graduates in the US—about 155,000, according to the Bureau of Labor Statistics—and you get an idea of the challenge.
Meanwhile, the industry is experiencing shortages of home health aides, nurse assistants, therapists, lab and imaging technicians, and other critical support people. Many nurses and other healthcare professionals fresh out of school are flocking to staffing agencies, which charge hospitals as much as three times full-time staff salaries for the temporary help, further siphoning the labor supply while crunching hospital budgets.
“The work is harder, the patients are sicker, and it's emotionally, physically taxing on the nurses and other personnel,” says Leslie Martin, chief nursing officer at Kingman Regional Medical Center, the largest healthcare provider in northwest Arizona. “Part of what we are struggling with is the competition to pay the high dollar prices that agencies can pay. It’s a lot easier to do a 13-week assignment and make as much as you can make in a whole year. A lot of hospitals are closing their doors because they can’t afford to continue paying these high prices.”
Policy proposals to boost the labor supply
All is not doom and gloom. Student enrollment in undergraduate nursing programs in the US increased by 3.3% in 2021 and is trending upward, despite concerns that the pandemic might discourage people from entering the profession, according to data released in April 2022 by the American Association of Colleges of Nursing. The number of students applying to US medical schools also ticked upward in 2021.
At the US national policy level, the AHA has called on lawmakers to enact or expand several measures to boost the supply of doctors, nurses, and other medical practitioners. Among its recommendations: increase financial support for nursing schools and faculty; increase funding for graduate medical education positions; fund more scholarships; forgive government-issued student loans (which can exceed a quarter of a million dollars just for a four-year med school education); expedite visas for highly trained foreign healthcare workers; and provide additional funding to address the behavioral health needs of overworked practitioners.
To their credit, most hospitals, clinics, hospices, urgent care centers, and other healthcare providers are taking matters into their own hands, strengthening their recruiting efforts, partnering with local education and training institutions, and creating more flexible, engaging work environments to improve employee retention.
For example, three hospital groups in Chicago—Advocate Aurora Health, Sinai Chicago, and University of Chicago Medicine—have launched a three-track program called the Bridge Initiative to recruit and develop workers at different levels of the healthcare profession. The program’s Healthcare Forward track, started with a grant from the JP Morgan Chase Foundation, offers high school students, mostly in economically depressed areas, free training and the guarantee of a job interview for entry-level positions. The Evolve track helps current employees advance their careers, while Rise Higher assists employees as they pursue careers in management.Under an innovative public-private partnership in Nova Scotia, Canada, CBBC Career College is working with local healthcare employers and the province’s Department of Seniors and Long-Term Care to prepare residents to become continuing care assistants (CCAs). Under the program, qualifying students will attend school three days a week tuition-free and work as paid CCAs two days a week, caring mostly for elderly clients in their homes or in assisted living facilities under the supervision of registered nurses.
Kingman Regional Medical Center is looking at creative ways to build a career path for its entry-level nursing assistants, including opportunities to receive scholarships and on-the-job training to become nurses or technicians—opportunities Kingman presents to internal and external candidates at its job fairs.
Flexible schedules and other incentives
Meanwhile, hospital groups are looking to attract and retain doctors, nurses, and other clinicians with a variety of incentives, including tuition reimbursement, childcare subsidies, and retention and merit bonuses. Some are paying their people daily or weekly rather than once or twice a month.
They’re also offering their people variable hours and part-time opportunities. Kingman has expanded its seasonal policy, whereby nurses can sign up to work stints of only three, six, or nine months a year. A parent, for instance, can choose to take the summer off to be with the kids. Kingman is also instituting a program under which it pays nurses a higher rate to work only on weekends.
Healthcare employers are offering some of their practitioners staggered start times as well as overlapping shifts to help with coverage. They’re even allowing some of them to set their own schedules, within certain parameters; an option that can appeal to young professionals and those with family responsibilities at home.
Some healthcare organizations are building or expanding their own internal staffing agencies to share practitioners across locations. Novant Health’s “float pool” of 200 or so nurses travel among the system’s 15 hospitals and 360 physician practices across the Carolinas. CHI Health is creating a reserve of nurses and therapists deployed among its 14 hospitals and hundreds of clinics across Nebraska.
In India, Apollo Hospitals is letting a number of specialists—in radiology, lab, endocrinology, palliative care, and other fields—work remotely, while creating a hybrid model for others, according to an article in The Economic Times. The tele-remote option has the added benefits of being more cost effective for hospitals, more convenient for many patients, and safer for caregivers and patients alike, especially amid infectious disease outbreaks.
Healthcare systems are training and educating caregivers to take on different or expanded roles. Nurse practitioners and physician assistants already have assumed some of the responsibilities that only doctors used to handle, such as diagnosing patient conditions and prescribing medications. Some of the work that was only performed by nurses, like drawing patients’ blood and giving them IVs, is also being spread to technicians. Many health systems have begun training “sideload workforces” to be able to take on specific critical-care and other responsibilities on short notice.
Tech solutions to operational challenges
But managing such a complex and nontraditional workforce can be its own clinical trial.
Oracle Executive Chairman Larry Ellison, who has made the healthcare industry a centerpiece of the company’s technology strategy with its recent acquisition of electronic health records (EHR) pioneer Cerner, has compared today’s healthcare providers to Uber, Airbnb, and other gig economy players. How so? Among their biggest operational challenges are recruiting, paying, scheduling, and evaluating an ever-changing pool of employees and contractors working variable hours from a variety of locations under different kinds of contracts and subject to different kinds of regulations.
Technology is playing a major role in helping healthcare providers manage those efforts, a major theme of the HIMSS 2023 Global Health Conference and Exhibition in Chicago April 17 to 21. For example, Adventist Health, which operates hospitals in California, Washington, Oregon, and Hawaii, used its new cloud-based human capital management (HCM) system to consolidate the 600 different ways it paid its nurses. Kingman Regional Medical uses ShiftWizard, a plugin to its Oracle Cloud HCM application, to let doctors and nurses self-schedule, capping the number who can sign up for a given shift.
Providers are also starting to tap the latest recruiting applications to identify job candidates most likely to fit in, perform at a high level, and stay at their organizations. Such applications can analyze LinkedIn and other data shared by job applicants—on their skills, credentials, work experiences, and interests—and correlate that data with the employer’s description of the open position’s requirements, as well as with data on recent hires with similar profiles who are succeeding at the organization.
Healthcare providers are also using workforce-planning applications to predict surges in patient demand and set doctors’ and nurses’ schedules accordingly. Northwell Health, one of the largest health systems in New York state, used a dashboard on its cloud-based HCM system to help its chief nursing officers stay abreast of patient inflows, staff recruitment, and resource requirements during the pandemic.
Cultivating the culture
Beyond using their HCM systems to simplify payroll, recruiting, and scheduling, healthcare organizations are tapping them to connect with, listen to, and motivate their people to reduce employee turnover, which is near an all-time high. The goal is to cultivate a work culture that makes employees feel more appreciated—and less inclined to seek opportunities elsewhere.
For example, healthcare providers are fielding “pulse surveys” from their HCM systems to solicit employees’ feedback on where they need the most support and on ways to improve the organization. They can then use the data collected in those surveys—augmented by more rigorous face-to-face workshops as well as one-on-one manager-employee conversations—to identify, discuss, and address concerns. Healthcare organizations are also using select HCM applications to connect burned-out caregivers with mental health services, while plugging their front-line people into communities of their peers for advice and support.
Robison, the former practicing nurse and now a health innovation scientist at Oracle, says healthcare providers need to get better at measuring how hard their nurses and other key people are working and where they’re spending their time, as a first step toward modifying their care delivery models to alleviate burnout. Data shows that certain routines can be simplified, automated, or offloaded to other employees, she says.
“We are building out a way to quantify all that work so that we can see how much time the patient requires and from whom,” Robison says. “That will allow administrators to make data-driven decisions about what the care teams need to look like. That's not something that we've been able to do in the past. Those decisions have been incredibly static.”
“We are building out a way to quantify all that work so that we can see how much time the patient requires and from whom. That will allow administrators to make data-driven decisions about what the care teams need to look like.”
Virtual care models offer alternative work options
EHR provider Oracle Cerner is working with clients to ease the burden on their nursing staffs by piloting a hybrid “virtual nursing” model. Under that program, an on-premises floor nurse orders and performs a physical assessment during a patient’s admission, while a nurse working over videoconference from home or at a hub in the building updates the patient’s data on allergies, medical history, and medications. Upon the patient’s discharge, the virtual nurse reviews orders and documentation, provides education, and checks if the patient’s pharmacy is documented. Some of that remote administrative work could be handed off to assistants.
Similarly, Kingman Regional Medical, which serves an aging population in rural Arizona, is considering implementing a program under which a nurse assistant would virtually monitor five or six patients from a central location, alerting hands on the floor to turn and lift patients and perform other taxing duties as needed, while freeing nurses for clinical care.
Technology is also helping healthcare providers rework their processes. After redesigning and automating its patient throughput processes using Oracle Cerner tools, the University of Tennessee Medical Center was able to cut in half the number of hours the full-time employees in its logistics center work.
Another major industry technology challenge is to make it easier for individual care providers to complete documentation and other administrative tasks. Doctors in 2021 spent an average of 15.6 hours per week on such tasks, according to the latest annual Physician Compensation Report from medical website Medscape. Children’s Minnesota hospital eliminated about 66 hours of clinicians’ EHR time per month just by standardizing and simplifying EHR processes.
Natural language speech-recognition software promises to minimize the time clinicians have to spend inputting data into EHRs and other systems. As for the output, it’s still hard for doctors and nurses to extract information from EHRs in real time to help them figure out what they need to do next. And because one vendor’s proprietary EHR system doesn’t always integrate with another’s, clinicians often can't even get all the information they need about a patient in one place, further complicating their workdays.
Improving health system connectivity, automation, and ultimately, patient outcomes is a much bigger challenge than any technology vendor can take on alone, Ellison noted during his keynote at Oracle CloudWorld in October. “We have to build a platform, not just a healthcare application or series of healthcare applications,” he said. “We can build some of those. But we have to build an open platform where others can innovate and plug in their technology.”
Building a talent pipeline
Even healthcare providers’ best programs and technology-based processes won’t do enough to alleviate the worker shortage absent a robust talent pipeline for them to tap into.
Building that pipeline in the US will require a national effort, says James Willig, a practicing physician and assistant dean of clinical education at the University of Alabama at Birmingham. That effort starts at the primary and secondary school levels to encourage academically gifted students—especially those from underrepresented ethnic groups and rural areas—to focus on the sciences and ultimately pursue a career in the medical fields, he says. Ongoing financial and academic support is key to cultivating that interest through the undergraduate and graduate levels, Dr. Willig says.
“You've got to keep growing those programs and those systems so that those kids can get there,” he says. “That’s true across healthcare—true for nursing, true for respiratory therapists, true for physical therapists. It starts early because you can't just say at the college level, ‘OK, we're going to give you a shot to go into medical school.’ Then it’s too late.”
It would be too easy to think that it’s never too late for healthcare providers to improve how they recruit, onboard, engage, motivate, and develop their key people. That’s until a lack of qualified personnel threatens a provider’s financial well-being—or worse, jeopardizes the health of a patient. The time to act is now.
-
Oracle Human Capital Management (HCM)
Oracle Fusion Cloud HCM is a complete cloud solution that connects every human resource process—and every person—across your enterprise. We help you create a community where people feel valued, heard, and like they belong.
-
Oracle Health
Oracle Health offers the most secure and reliable healthcare solutions, which connect clinical, operational, and financial data to improve care and advance decision-making around health and well-being.